
Genetics. Whew! For Ehlers-Danlos Syndrome it’s gold standard. For hypermobile Ehlers-Danlos, it’s nearly impossible to SEE the geneticist nowadays, and Classic EDS isn’t far behind. The reason is because of the influx of patients demonstrating clearly to geneticists and gen clinics that there are too many people to handle in a category that can no longer be considered rare. Unfortunately, as clinics shut their doors to all but the most severe and obvious cases of EDS, there remain no other specialists to pick up the slack leaving families like ours to coordinate and direct ALL of the care.
We have been able to create a paper trail of symptoms for our children and advocate successfully to get our son to an excellent peds geneticist very quickly. It was an educational process! We had to learn what to document, how to find and encourage an EDS education for our primary, and how to present the sets of symptoms to her as EDS plus multisystem co-conditions with the vocabulary and context the symptoms need to stand out. Our primary was very quick to diagnose hypermobility spectrum disorder to get us started, and has been on the ball for any referrals we have needed, including genetics with Atrium Health in Charlotte, NC.
Side NOTE: While we were working on this project, several of the physicians here in North Carolina who specialize in different components of EDS have been sharing with me their view on the current state of the genetics focus and their view of what the future for EDS care will look like. They voiced how little geneticists can actually do, even IF a gene for hEDS is found. They expressed the sincere wish that parents would seek treatment from knowledgable EDS and hypermobility providers with more urgency, leaving genetics till later or putting it off completely unless there is substantial evidence for Classical, Vascular and other rare forms of EDS. And our recent experience with this excellent peds geneticist shows WHY.
We’ve been to see him twice. Our first visit in the spring was positive! He ran a test to rule out a big alternative in my son’s case called Stickler Syndrome, which can present early with Pierre Robin Sequence (a genetic malformation of the jaw and placement of the tongue in utero with other implications) as it can in Ehlers-Danlos Syndromes too. We left awaiting results, and the promise to evaluate for EDS when he was older if symptoms persisted. He was 8 at the time and is now 9 years old. Since we already had a medical team treating “symptomatic hypermobility spectrum disorder” this wasn’t an issue. My primary goal for a genetics diagnosis in Sam’s case is to streamline future care. When his spine symptoms worsened this summer impacting posture, pain and vision, and some new family history came to light with a slew of EDS related symptoms and some diagnoses of co-conditions, we reached out for a second visit. Here’s how it went.
Sam does not meet the criteria for diagnosis based on the Beighton Score. The Beighton Score is law for hEDS diagnosis by a geneticist and so Sam could not be diagnosed by a geneticist who wants to follow the rules. He does not meet the Beighton because of muscle contractures in his legs, and because his thumbs and wrists are not very hypermobile (he does get pain, popping and burning in ALL of his joints in a flare). Using articles showing the prevalence of dystonias in EDS patients and the impact of deep contractures on diagnosis, I made the case that it only takes 1-2 seriously hypermobile joints to make an accurate diagnoses of hypermobile Ehlers-Danlos Syndrome when other multisystem symptoms or diagnosed conditions are also present (Hamonet, et al). This doctor agreed with me, and recommended that we see one of a list of EDS specialists who does not have to abide by the laws that geneticist have to abide by.
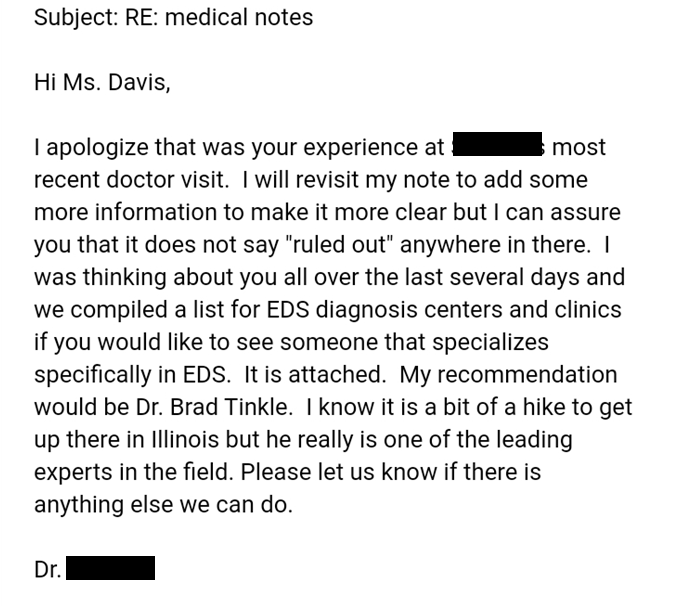
Here is a screen shot of the message he sent me when, a day later, I had an encounter with another physician who felt that his notes indicated that he thought Sam did NOT have EDS.
So what is my take away from all of this? First, and very important! There ARE genetic conditions that can occur WITH hEDS and the other types, or that might be in place of EDS, and you do need a geneticist to rule those out or confirm them. It is a rare combination, however, so the more you can learn about EDS and your child’s symptoms, the better position you will be in to determine whether advocating for genetic testing is worth the time and expense. Second, until the committee meets again to establish new diagnostic criteria in light of new research and clinical studies occurring around the world in relationship to Ehlers-Danlos Syndromes, the best thing you might be able to do as a parent or patient is to seek out EDS aware specialists for treating symptoms, and who might know how to make the hEDS diagnosis in place of the geneticist.
Here are some tips:
- Learn as much as you can about Ehlers-Danlos, Hypermobility Spectrum disorders, and the co-conditions of EDS.
- See the resource page for patients, books like Disjointed by Diana Jovin, and ECHO Events with the Ehlers-Danlos Society (scholarships usually available!).
- Learn how to observe the symptoms and document them in different contexts so that your reports to your primary care provider can positively indicate EDS and the co-conditions.
- For example: once you know the symptoms of dysautonomia, you can begin to notice how your child reacts to temperature changes, has odd level fatigue in heat compared to other children, check HR at random times every 6 months or so and see if it’s too high for the activity, not returning to normal, and other early signs you can learn to recognize quickly from the literature.
- When symptoms become obvious enough, change from irregular to intermittent or intermittent to regular, (please don’t wait for it to move from regular to CONSTANT if you strongly suspect EDS!), have the primary document and then refer you to an EDS knowledgable specialist in the area you need.
- Cardiology
- Immunology/Allergy
- Gastroenterology
- Spine Specialist and Neurosurgeon
- Neurology
- Physical AND Occupational therapy
- Sleep Specialists
- And more, wonderfully categorized by Diana Jovin in Disjointed and those in categories described on the patient resources section of this website.
- When you present your concerns to the specialist, note that it is there job to rule out other possible conditions. If you have become knowledgable yourself about the co-conditions of that same discipline, you can advocate for the tests needed in a case of EDS to be done at the same time. Also, in most cases you cannot expect a doc to do that by default even if they are known to treat EDS patients. Go prepared to ASK for specific tests, or how to document symptoms they need for observational diagnosis.
- For example, in MCAS the most helpful positive diagnostic is a tryptase blood test and n-methylhistamine in the urine. Tryptase requires a baseline measurement (non-flare) with a 20%+2 elevation in a flare plus symptoms for MCAS diagnosis. Having your primary test for baseline tryptase, or making sure the allergist tests for these at the same time as a skin prick, can establish that baseline for future possible MCAS progression.
- If you’ve had to get all the way to this point then you are likely on the right track and learning just how much work it is to manage a multi-system condition. You may at this time seek a geneticist, but be aware of your expectations! You might get lucky and get the hEDS diagnosis if your child meets the Beighton. If not, you can learn about deep muscle contractures, signs and symptoms, and go prepared to request the connective tissue panel “for peace of mind.” There ARE related mutations that can indicate EDS as a “maybe”. You run the risk of having the geneticist officially rule out EDS, but with preparation you can be specific about asking them NOT to rule it out for the following reasons.
- The Beighton is increasingly known to be inaccurate. It was actually never meant to be a diagnostic RULE, only a tool of observation.
- A Beighton score is impossible in a child or adult with deep muscle contractures, and possible cord tethering restricting the legs deep down beneath the muscle (children with this may complain of frequent non-joint leg pain and pulling in the soles of the feet also).
- Genetic and genetically diagnosable can be very different! If symptoms suggest more severe connective tissue issues, or other genetically diagnosable conditions from your family history, go prepared to address ALL of it. Focusing only on EDS can backfire based on the bias or rules of the geneticist you see. If you have multiple issues that suggest genetically diagnosable problems, come with all of them.
Most early symptoms of hypermobility spectrum disorders have natural interventions that good doctors will seek out before medications. These include increasing healthy salt intake and LOTS of water, compression clothing around the thighs and core for both dysautonomia and proprioception difficulties (loosing balance, running into things, falling), anti-inflammatory diets which do not restrict foods but exchange inflammatory foods for those less irritating (gluten free is very common, followed by dairy free, and anti histamine which you can read more about here). These and much much more you can read about in my Cultural Approach to Long Term Stability and accompanying handout, including how to find good PT’s and OT’s for your kids, and ALL of this can be monitored and managed by your primary care provider.
While genetics has been designated as necessary for the time being, the research being done at the GLOBAL level for treating connective tissue disorders and hypermobility spectrum disorders are going to bring about major changes for our community. You are your own, and your children’s, BEST advocate. And you know where to find me if you need help and support.
All the best,
Rachel Lee